Chapter Five: Functions of the Distal Nephron
Chapter Five: The Distal Nephron is the Best Nephron.
References for Chapter 5--the Distal Nephron
Roger pointed out the fact that the distal nephron can achieve very low urinary sodium as evidenced by observations in people from the Yanomamo tribe Blood pressure and electrolyte excretion in the Yanomamo Indians, an isolated population in this report, 84% of the participants had urinary sodium < 1mmol/24 hours.
Information about the Yanomamo Tribe. It looks like they’re starting to make chocolate, now!
I believe this is the original study looking at urine sodium and blood pressure in the Yanomamo Indians, but the INTERSALT trial linked above I believe had more robust urine data
This study mentions the average lipid profile for men and women along with BMI.
I didn’t mention in the “Voice of God” overview, but there is some interest looking at the Yanomamo and rate of cancer as it relates to the correlation with intracellular potassium to sodium ratios
Josh referred back to his notes and realized that the tightest junctions are in the TOAD not FROG bladders Physiology and Function of the Tight Junction
An excellent review from McCormick and Ellison on the Distal convoluted tubule in Comprehensive Physiology.
We flirt with the disorder of Gordon’s syndrome: Familial Hyperkalemic Hypertension | American Society of Nephrology and its alter ego, Gitelman syndrome: Gitelman Syndrome | Hypertension
JC spoke about this beautiful report on how calcineurin inhibitors lead to hyperkalemia (and mimic Gordon’s syndrome). The calcineurin inhibitor tacrolimus activates the renal sodium chloride cotransporter to cause hypertension
This superb review of the DCT includes all the highlights of Rose’s chapter 5 with a modern lens including “braking” from DCT hypertrophy Distal Convoluted Tubule | American Society of Nephrology
Echos of the lessons learned in the DCT can be seen in this review: Diuretic Treatment in Heart Failure | NEJM
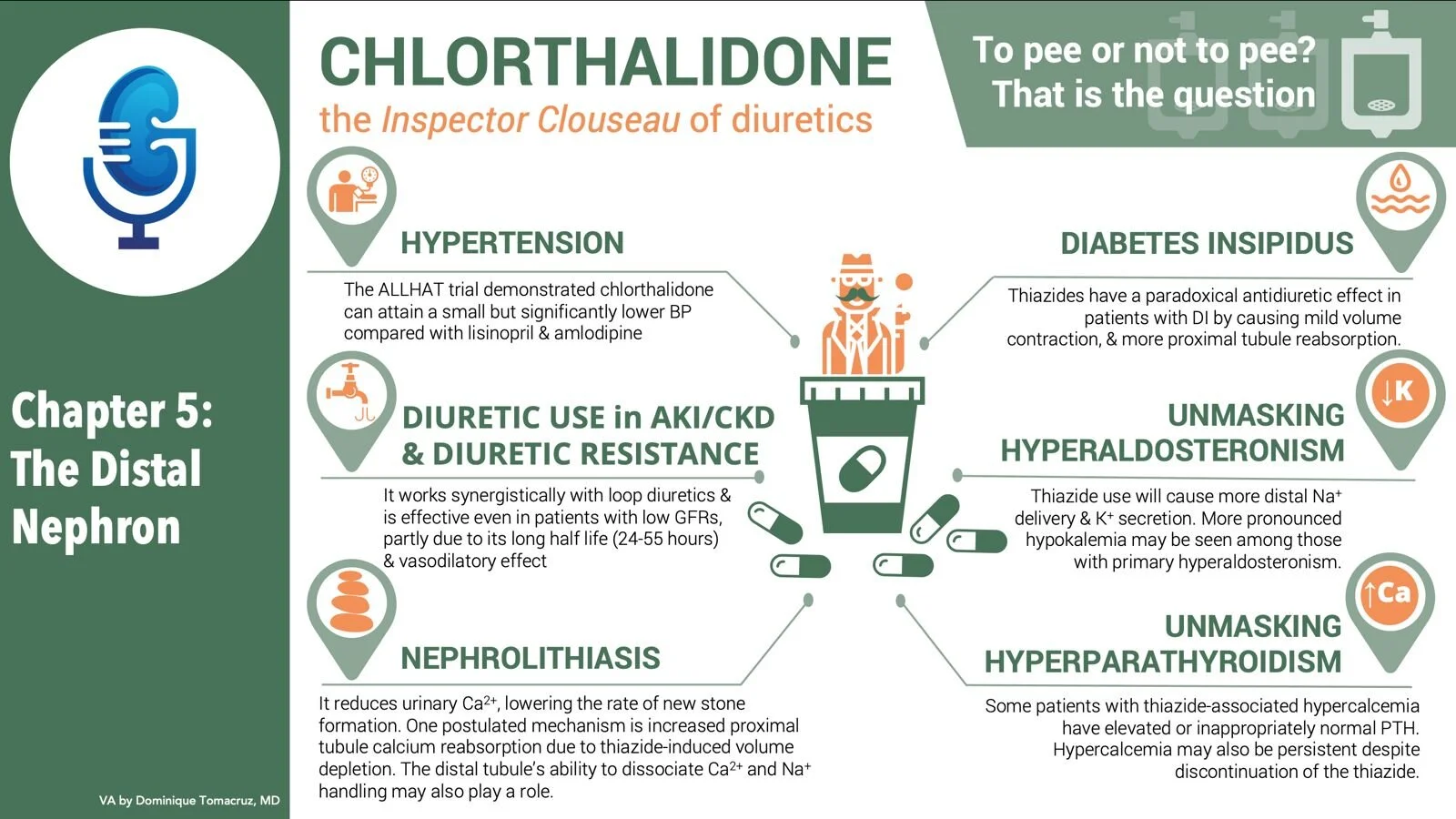
Anna reminds us of the ALL HAT trial which showed that chlorthalidone was superior to the lisinopril and amlodipine groups (and the alpha blocker dropped out earlier) Major Outcomes in High-Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
Nice review of drug induced Hyperuricemia with a deep dive into the mechanisms of diuretic induced Hyperuricemia. Drug-induced hyperuricaemia and gout
Plus, despite the concerns that thiazides are weaker than loop diuretics and may not work in CKD, this report suggests that it can still be of use. Chlorthalidone for poorly controlled hypertension in chronic kidney disease: an interventional pilot study
If you love diuretics, you will love this classic paper from Craig Brater on diuretics Diuretic Therapy | NEJM which also includes the t1/2 of various diuretics and points out that chlorthalidone’s half life is 24-55 hours so eliminated after 4-10 days.
The hypercalcemia seen in some patients who take thiazides may be the unmasking of primary hyperparathyroidism Thiazide-Associated Hypercalcemia: Incidence and Association With Primary Hyperparathyroidism Over Two Decades
As we discussed the relative importance of DCT vs Proximal tubule for the hypercalcemia seen with thiazides, Amy reminded us of about the TRPV5 knockout mice: JCI - Renal Ca2+ wasting, hyperabsorption, and reduced bone thickness in mice lacking TRPV5
JC mentioned the defect in TRPM6 that can cause severe hypomagnesemia: Novel TRPM6 Mutations in 21 Families with Primary Hypomagnesemia and Secondary Hypocalcemia
We enjoyed talking about Liddle syndrome Hypertension caused by a truncated epithelial sodium channel γ subunit: genetic heterogeneity of Liddle syndrome
We wondered about the role of pendrin which was discovered after this book was published. Here’s a nice review: The role of pendrin in renal physiology and also a potential therapeutic target for pendrin: Pendrin—A New Target for Diuretic Therapy? | American Society of Nephrology
More Bradykinen Chronic Overexpression of Bradykinin in Kidney Causes Polyuria and Cardiac Hypertrophy
We ended on a high note when we considered the urothelium of the American black bear. These magnificent creatures have aquaporins 1 &3 that allow them to reabsorb their own urine during hibernation. The urothelium of a hibernator: the American black bear
Outline: Chapter 5
- Functions of the distal nephron
- Begins at the macula densa at the end of the cortical thick ascending limb
- Four segments
- Distal tubule
- Connecting segment
- Cortical collecting tubule
- Medullary collecting tubule
- Site of final qualitative changes in urine excretion are made
- Urinary concentration
- Urinary acidification
- Secretion of potassium
- Sodium conservation
- Sodium enters the distal nephron at 75 mEq/L and can exit the kidney at <1 mEq/L
- Very thick tight junctions
- 8 strands (only 1 strand in the proximal tubule)
- Prevents back diffusion of solutes and water into the tubule (and vice versa) the paracellular route is closed off.
- Three processs protect the distal nephron from seeing massive amounts of fluid
- Autoregulation
- TG Feedback (typo, in should be if)
- GT balance
- Great line “In General cellular function correlates closely with hormonal responsiveness”
- Na resorp and K secretion with Aldo responsiveness
- Water resorption in ADH responsive cells
- Ca resorption in cell responsive to PTH and calcitriol
- And there is intercalated cells that don’t really fit, respond primarily to pH and minimally to aldo
- Distal Tubule (seems like this should be called DCT)
- Sodium and water
- Reabsorbed 5% of of filtered NaCl
- NaCl co-transporter
- Powered indirectly by NaK-ATPase
- Which keeps intracellular Na low and intracellular charge Negative
- The negative charge unimportant in DCT where resorption is electro neutral
- In addition to NaCl co-transporter, also parallel exchanger
- H secreted and Na reabsorbed
- HCO3 secreted and Cl reabsorbed
- H and HCO3 reform to neutral carbonic acid and moves intracellular
- Mentions gitelman syndrome
- Na reabsorption is dependent on Na delivery so this participates in Glom Tubule Balance
- So the common phenomenon of increased DCT Na resorption with loop diuretics can be described as another example of GT balance.
- This is maladaptive with high Na diet where increased (and appropriate) Na delivery results in increased (and maladaptive) Na reabsorption.
- The key sites of regulation are the proximal and collecting tubule
- Regulated by
- Aldosterone
- AT2
- ANP
- Water handling
- Water impermeable
- Unresponsive to ADH
- A member of the diluting segments
- Calcium
- DCT has Ca resorption capability, increased by PTH
- Increased calcium suppresses PTH and reduces Ca reabsorption here
- Na and Ca reabsorption can be disassociated in the DCT
- Connecting segment
- Hybrid DCT and CCD
- Impermeable to water and ADH unresponsive
- Reabsorbed Ca and is responsive to both PTH and calcitriol
- Has NaCl cotransporter as well as eNaC
- Secretes K in response to aldo
- Cortical collecting tubule
- Principal cells
- Na flows down its electrical gradient into the cells
- The interior of the cell is negative due to the activity of
the 2K 3Na ATPase (also aided by K leaking out, further lowering interior charge)
- Negative charge is essential since tubular Na goes below interior Na concentration
- The electrogenic movement of Na leaves the tubule negative which promotes:
- Chloride paracellular reabsorption
- Potassium secretion
- Increased Na diet which increases Aldo
- Increases sodium channels from < 100 to around 3000
- Liddle syndrome is an activating mutation of eNaC
- Autosomal recessive pseudohypoaldosteronism is a inactivating mutation
- Says must of the dietary changes in sodium intake are regulated here
- Mostly Aldo dependent possibly some ANP effect
- Water handling
- Water impermeable in basal state
- Responds to ADH with aquaporin 2 channels
- Tubular fluid here has osmolality of 100 compared with the body at 300, so brisk passive movement from the tubules.
- Water resorption decreases tubular flow but this doesn’t affect potassium secretion since ADH stimulates the addition of more K channels
- An aside about lithium
- Intercalated Cells
- Na independent regulation of acid-base
- H enters the lime from H-ATPase or a H-K-ATPase
- Then Cl-HCO3 exchanger removes the HCO3 from the cell
- Aldosterone is permissive (what does this mean?)
- Though hyperaldo does cause metabolic alkalosis
- If there is an alkali load intercalated cells can secrete bicarb
- Reversed polarity type A cells forms type B cells
- Can reabsorb K in hypokalemia
- H-K-ATPase reabsorbs K
- Found in type B and A cells
- Unresponsive to ADH
- Impermeable to water
- Medullary collecting tubule
- Transition from medullary to cortical is not abrupt
- In the late two thirds of medullary collecting tubule it is mostly a unique cell type that sounds like a principal cell but is described differently
- It reabsorbs Na through an amino ride sensitive channel
- But rather than a lot of K secretion, sounds like a lot more chloride resorption
- Water resorption is driven by ADH but there is additionally...
- A lot of urea absorption stimulated by ADH
- Location of urea resorption for urea cycling